Genetic factors shape fertility outcomes more than most people realize. Roughly 15% of infertility cases stem directly from chromosomal abnormalities or gene mutations in either partner, yet many patients enter IVF without a clear picture of how their DNA influences their chances. Understanding the role of genetics in IVF means knowing which tests exist, what they can and cannot tell you, and how that information guides the decisions your care team makes. This article explains all of it clearly, from the genetic roots of infertility to the ethical questions surrounding embryo screening.
Table of Contents
- Key takeaways
- The role of genetics in IVF starts before conception
- Genetic testing methods used in IVF
- Challenges and ethics of genetic screening in IVF
- How genetics shapes IVF treatment decisions
- My perspective on genetics and IVF after years in this field
- How Lifeivfcenter integrates genetics into your IVF care
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Genetics and infertility | About 15% of infertility cases have a direct genetic cause in one or both partners. |
| PGT screening types | PGT-A, PGT-M, and PGT-SR serve different purposes and are selected based on each patient’s profile. |
| Test limitations matter | No genetic test predicts IVF success with certainty; results require careful clinical interpretation. |
| Counseling is non-negotiable | Expert genetic counseling helps you interpret uncertain results and make informed transfer decisions. |
| Personalized protocols win | Integrating genomic data into IVF planning improves embryo selection and reduces unnecessary cycles. |
The role of genetics in IVF starts before conception
Before a single embryo is transferred, genetics is already at work. Both male and female infertility can trace back to chromosomal or molecular disruptions that standard fertility workups sometimes miss entirely.
Chromosomal abnormalities and structural rearrangements
Chromosomal problems fall into two broad categories: numerical errors (having too many or too few chromosomes, called aneuploidy) and structural errors (pieces of chromosomes that are deleted, duplicated, or rearranged). Either type can prevent fertilization, cause early miscarriage, or result in embryos that simply fail to implant. Women with recurrent pregnancy loss often carry a balanced chromosomal translocation, meaning their own chromosomes are rearranged but functional. The problem emerges when those rearrangements are passed to embryos in unbalanced forms.
Single gene mutations and male-specific factors
Single gene mutations contribute to conditions like cystic fibrosis, spinal muscular atrophy, and fragile X syndrome, all of which are relevant to reproductive planning. On the male side, Y chromosome microdeletions affect regions of the Y chromosome critical to sperm production, causing severe oligozoospermia (very low sperm count) or azoospermia (no sperm at all). These deletions are not detectable through a standard semen analysis.
Beyond chromosomes and genes, epigenetic mechanisms also matter. Epigenetics refers to changes in how genes are expressed without altering the underlying DNA sequence. Epigenetic disruptions in male infertility can affect sperm quality, fertilization rates, and embryo development in ways that only emerge after IVF cycles begin.
The key genetic causes of infertility include:
- Aneuploidy: Extra or missing chromosomes in eggs or sperm
- Balanced translocations: Rearranged chromosomes that cause unbalanced embryos
- Y chromosome microdeletions: Genetic deletions disrupting sperm production in men
- Single gene disorders: Mutations inherited from one or both parents affecting reproductive function
- Epigenetic changes: Altered gene expression patterns affecting embryo viability
Pro Tip: If you or your partner has a family history of a known genetic disorder, ask your physician about carrier screening before starting IVF. Knowing your carrier status early shapes every downstream decision.
Genetic testing methods used in IVF
Understanding how genetic screening works in IVF requires knowing that there are multiple distinct test types, each designed to answer a different clinical question. These are grouped under the umbrella of Preimplantation Genetic Testing, or PGT.
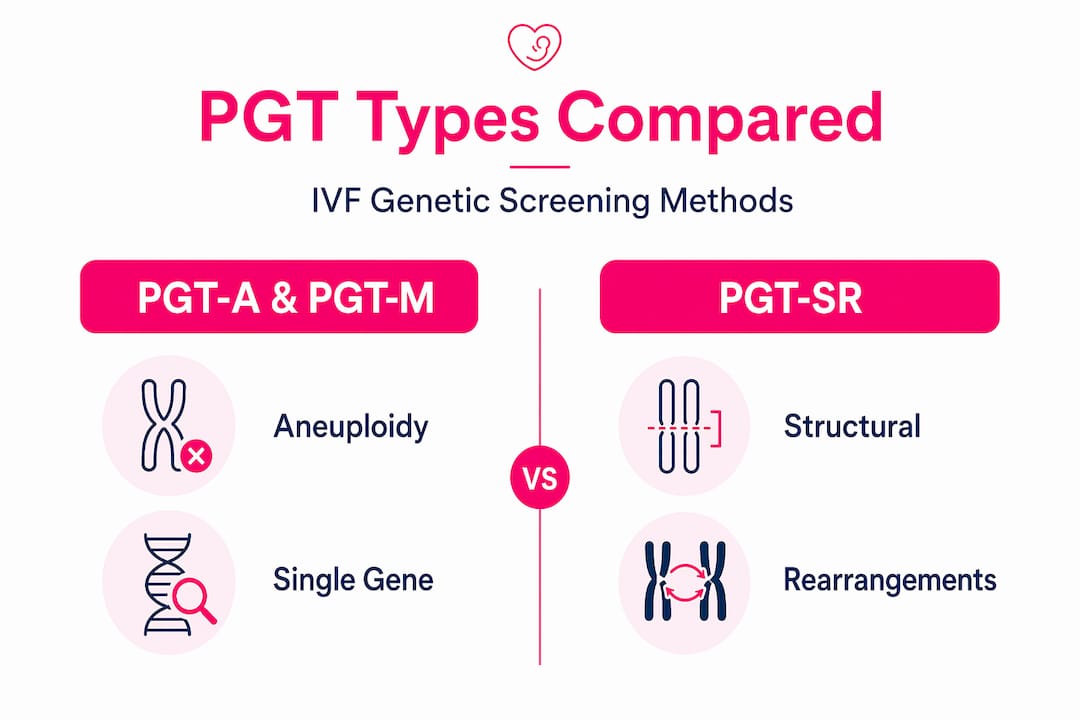
The three main PGT types explained
Multiple PGT types are used at various stages of the IVF workflow to support personalized embryo selection. Here is how they differ:
| PGT Type | Full Name | What It Screens For |
|---|---|---|
| PGT-A | Preimplantation Genetic Testing for Aneuploidy | Chromosome number errors (too many or too few) |
| PGT-M | Preimplantation Genetic Testing for Monogenic Disorders | Specific single gene mutations (e.g., BRCA1, cystic fibrosis) |
| PGT-SR | Preimplantation Genetic Testing for Structural Rearrangements | Chromosomal translocations or inversions |
Each test requires an embryo biopsy, typically performed on day 5 or 6 when the embryo has reached the blastocyst stage. A small number of cells are removed from the outer layer of the embryo (the trophectoderm, which becomes the placenta) and sent for DNA analysis. The embryo itself is frozen while results are processed, usually within one to two weeks.
How DNA analysis works in the lab
Once the biopsied cells reach the lab, next-generation sequencing (NGS) is the most widely used platform for analysis. NGS reads thousands of DNA fragments simultaneously to detect chromosomal imbalances, specific mutations, or structural changes. For male infertility cases, NGS panels can achieve diagnostic yields up to 40% in severe cases, identifying genetic causes that routine semen analysis would never detect.
Carrier screening, which tests parents rather than embryos, is typically completed before IVF begins. Both partners submit blood or saliva samples to check whether they carry mutations for recessive disorders. If both partners carry a mutation for the same condition, PGT-M becomes highly relevant for embryo selection.

Emerging technologies worth watching include non-invasive PGT, which analyzes spent culture media (the fluid embryos develop in) rather than biopsied cells, and whole genome sequencing, which provides a far broader genetic picture. Both are still being validated for clinical use but represent the direction the field is heading.
Pro Tip: PGT-A test performance varies significantly by laboratory platform and the clinical team’s experience interpreting results. Always ask your clinic which sequencing platform they use and what their validation data shows.
Key benefits of genetic testing in IVF include:
- Identifying chromosomally normal embryos for transfer, reducing miscarriage risk
- Detecting carriers of serious hereditary diseases before embryos are created
- Guiding treatment decisions for couples with structural chromosomal rearrangements
- Informing sperm selection decisions in severe male factor infertility cases
Challenges and ethics of genetic screening in IVF
The role of genetic screening in IVF is not without complexity. Genetic information is powerful, but it also introduces clinical uncertainty and ethical questions that deserve honest consideration.
Variants of Uncertain Significance create real dilemmas
One of the most underappreciated challenges in genetic testing is the Variant of Uncertain Significance, or VUS. A VUS is a genetic change detected in a test result that science has not yet classified as clearly harmful or benign. Many infertility gene variants remain VUS with limited functional evidence to guide clinical decisions. Receiving a VUS in your results can feel alarming, but acting on it aggressively without evidence often does more harm than good.
The ethical concerns surrounding broad genetic screening include:
- Risk of discarding viable embryos: Mosaicism (a mix of normal and abnormal cells in one embryo) can lead to false positives, potentially causing clinicians to discard embryos that could have developed into healthy babies
- Equity gaps: Genetic testing adds cost that not all patients can absorb equally
- Over-testing pressure: Broad PGT-A application has not been shown to significantly improve IVF success rates across all patient populations
- Psychological burden: Waiting for genetic results while embryos are frozen is emotionally taxing, and receiving a “no normal embryos” result can feel devastating
“The decision to pursue genetic testing during IVF involves complex considerations that require expert clinical guidance, informed consent, and careful attention to each patient’s values and circumstances.” — ACOG, 2026
Expert genetic counseling is not optional in this context. Patients who receive genetic results without adequate counseling often misinterpret what those results mean for their specific situation, leading to decisions made under unnecessary anxiety rather than informed clarity.
How genetics shapes IVF treatment decisions
When genetic data is used thoughtfully, it can genuinely improve outcomes. The impact of genetics on fertility treatment extends beyond simply identifying problems. It reshapes the entire protocol.
Here is how genetic insights translate into clinical decisions during IVF:
- Embryo prioritization: PGT-A results allow physicians to rank embryos by chromosomal status, transferring euploid (chromosomally normal) embryos first. This reduces miscarriage rates and improves the probability of a live birth per transfer.
- Tailored stimulation protocols: Integrated genomic and AI-driven data increasingly inform how physicians adjust ovarian stimulation dosing based on a patient’s biological profile, including genetic markers related to ovarian reserve.
- Male factor decisions: When severe male factor infertility has a known genetic cause, such as a Y chromosome microdeletion, the care team can counsel the couple that any male children may inherit the same deletion. This is critical information for informed consent before using that sperm for IVF. Understanding male factor infertility’s genetic causes allows couples to make decisions grounded in facts rather than uncertainty.
- Preventing hereditary disease transmission: PGT-M allows couples who are carriers of serious conditions like Huntington’s disease or sickle cell anemia to select unaffected embryos for transfer, preventing the condition from being passed to their child.
- Informing donor considerations: If genetic testing reveals that a patient is unlikely to produce chromosomally normal embryos with their own eggs, that data supports a more direct conversation about donor egg options, sparing patients unnecessary cycles.
PGT-A predictive accuracy depends heavily on which platform a clinic uses and how experienced their embryologists are at interpreting borderline results. This is why centralized, specialized fertility centers tend to produce more reliable outcomes from genetic testing than generalist practices.
Pro Tip: Ask your clinic how they handle mosaic embryo results. Clinics with strong genetic counseling programs will have a clear, evidence-based policy for discussing and transferring mosaic embryos rather than defaulting to discarding them.
My perspective on genetics and IVF after years in this field
I’ve worked alongside patients navigating genetic testing results long enough to have seen the same pattern repeat itself. The numbers on a lab report land hard, and people often make the most important decisions of their reproductive lives in a state of shock rather than clarity.
What I’ve learned is that the most harmful thing in this process is not a bad result. It’s a result delivered without context. I’ve seen couples abandon a viable embryo transfer because a mosaic result scared them, when the clinical evidence would have supported a cautious transfer. I’ve also seen the reverse: patients push for transfer of embryos that genetic counseling would have flagged as high-risk, because no one took the time to explain what the result actually meant.
The promise of genetic testing in IVF is real. Genetic factors in assisted reproduction are now understood well enough that we can meaningfully reduce miscarriage rates and prevent heritable diseases. But the caution is equally real. Testing technology moves faster than clinical interpretation expertise, and not every lab or clinic has the experience to translate results into genuinely personalized guidance.
My honest advice: prioritize the quality of your counseling as much as the quality of your testing. A result is only as useful as the clinical team that helps you understand it.
— Ben
How Lifeivfcenter integrates genetics into your IVF care
If you are exploring IVF and want genetic testing built into your treatment from the start, Lifeivfcenter offers exactly that through its Precision IVF approach, which customizes your protocol based on your biological profile, genetic history, and reproductive goals.
Genetic screening, carrier testing, and PGT integration are part of how Lifeivfcenter works to reduce unnecessary cycles and improve live birth rates for each patient. The clinic also provides access to counseling support so you are never left interpreting a result on your own. If cost is a concern, transparent fertility treatment packages make it easier to plan your care without financial surprises. Reach out to schedule a consultation and find out what a genetics-informed IVF plan could look like for you.
FAQ
What is the role of genetics in IVF outcomes?
Genetics influences which embryos are viable for transfer, whether hereditary diseases are passed to a child, and how treatment protocols are personalized. Chromosomal abnormalities are a leading cause of implantation failure and early miscarriage, making genetic screening a meaningful tool in improving IVF success.
What does PGT-A test for in IVF?
PGT-A screens embryos for aneuploidy, meaning chromosomes that are present in the wrong number. Transferring chromosomally normal embryos reduces miscarriage risk and can improve live birth rates per transfer cycle.
Can genetic testing guarantee IVF success?
No. PGT-A test performance varies by platform and lab, and no current test predicts IVF success with certainty. Genetic testing improves decision-making but does not eliminate all variables affecting implantation and pregnancy.
What is a Variant of Uncertain Significance in fertility testing?
A Variant of Uncertain Significance, or VUS, is a genetic change detected in testing that cannot currently be classified as harmful or benign. Many infertility-related gene variants fall into this category, which is why genetic counseling is critical before acting on any result.
Who should consider genetic testing before or during IVF?
Couples with a known hereditary condition, recurrent pregnancy loss, severe male factor infertility, advanced maternal age, or a previous child with a chromosomal condition are strong candidates for genetic testing as part of their IVF care plan.
Recommended
- The Role of Technology in IVF: What Really Works
- Endometriosis IVF Process: What You Need to Know
- IVF Process Explained: Personalize Your Path to Success
- A. Intro to IVF Archives – Life IVF Center
Ready to take the next step?
Life IVF Center specializes in individualized Precision IVF® care for complex cases—including diminished ovarian reserve, prior failed cycles, and advanced maternal age. Our in-house labs and dedicated physicians are ready to help.
Book a Free Consultation →