For women with endometriosis, the path to pregnancy is rarely straightforward. The endometriosis IVF process requires more than a standard treatment plan. It demands a protocol built around your specific disease stage, ovarian reserve, and inflammatory profile. Roughly 30 to 50 percent of women with endometriosis face infertility challenges, yet many go on to have successful pregnancies with the right IVF approach. This article walks you through every phase of IVF tailored for endometriosis, from preparation and protocol selection to transfer timing and realistic success expectations.
Table of Contents
- Key takeaways
- Understanding endometriosis and fertility before IVF
- Customized IVF protocols for endometriosis patients
- The IVF process step by step for endometriosis
- Success rates and outcomes based on endometriosis stage
- My perspective on IVF with endometriosis
- How Lifeivfcenter supports endometriosis patients
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Staging shapes your protocol | Your rASRM disease stage directly influences stimulation choices, egg yield expectations, and transfer strategy. |
| Freeze-all is often preferred | Frozen embryo transfer consistently outperforms fresh transfer in endometriosis patients by allowing inflammation to settle. |
| Surgery before IVF is not always right | Removing endometriomas can reduce ovarian reserve, so surgery should only proceed when cysts block follicle access. |
| Protocol customization matters | GnRH antagonist protocols are now preferred for safety, but gentler options like mini-IVF may suit some patients better. |
| Success rates vary by stage | Stages I and II see outcomes comparable to women without endometriosis, while stages III and IV require adjusted expectations. |
Understanding endometriosis and fertility before IVF
Endometriosis affects fertility through several overlapping mechanisms. Scar tissue and adhesions distort pelvic anatomy, impairing egg pickup and embryo transport. Chronic inflammation creates a hostile environment for eggs and embryos. And perhaps most significantly, endometriomas on the ovaries can progressively damage ovarian tissue, reducing your egg reserve over time.
Before starting IVF for endometriosis, your care team will assess several key factors:
- Ovarian reserve tests, including AMH (anti-Müllerian hormone) and antral follicle count, to gauge how many eggs you are likely to produce
- rASRM staging (stages I through IV), which classifies disease severity based on lesion depth, location, and the presence of adhesions or endometriomas
- Pelvic ultrasound and imaging to identify endometriomas and structural changes
- Surgical history, since prior ovarian surgeries can affect reserve and complicate retrieval
The rASRM stage matters more than most patients realize. ART outcomes are similar to non-endometriosis controls in stages I and II, while advanced stages III and IV show measurable reductions in egg retrieval numbers, clinical pregnancy rates, and live birth rates. Knowing your stage informs every decision that follows.
The NICE endometriosis fertility pathway recommends advancing to IVF discussion after two years if expectant management or surgery has not resulted in pregnancy, with earlier consideration when age, ovarian reserve, or symptom severity warrants it. This guidance prioritizes individualized decision-making rather than a fixed timeline.
You can use a thorough fertility evaluation checklist to prepare for the clinical workup your specialist will likely order before your first IVF cycle.
Customized IVF protocols for endometriosis patients

Not all IVF protocols are created equal, and this distinction matters most for women with endometriosis. The two major stimulation approaches are GnRH antagonist and GnRH agonist (long protocol) regimens, and the field has shifted considerably in recent years.
| Protocol | How it works | Best suited for |
|---|---|---|
| GnRH antagonist | Suppresses premature ovulation quickly; starts stimulation early in cycle | Most endometriosis patients; lower OHSS risk |
| Long GnRH agonist | Suppresses ovaries over weeks before stimulation begins | Some advanced-stage patients needing deep suppression |
| Progestin-primed (PPOS) | Uses oral progestin alongside FSH to prevent early LH surge | Patients seeking a gentler, more flexible cycle |
| Mini-IVF | Lower-dose stimulation targeting fewer, higher-quality eggs | Women with diminished reserve or medication sensitivity |
GnRH antagonist protocols are now preferred over long agonist protocols because they produce comparable pregnancy rates with fewer side effects and a lower risk of ovarian hyperstimulation syndrome (OHSS). For women whose ovarian reserve is already compromised by endometriosis, avoiding OHSS is not just a comfort consideration. It is a medical priority.
Mini-IVF and PPOS protocols offer a gentler alternative worth discussing with your doctor. PPOS separates stimulation from embryo transfer entirely, which many patients with active symptoms find easier to manage physically and emotionally. You can read more about this option in Lifeivfcenter’s guide to mini-IVF benefits.
One of the more nuanced decisions in preparing for IVF with endometriosis involves endometriomas. The general recommendation is to defer surgical removal unless a cyst is large enough to physically block follicle access during retrieval. Surgery before IVF can reduce ovarian reserve, sometimes significantly, so the calculus must weigh symptom relief against fertility impact. When surgery is unavoidable, fertility preservation through egg or embryo freezing beforehand is strongly advised.
Pro Tip: Ask your specialist specifically about a 2 to 3 month pre-treatment course of GnRH analogues. Some clinics use this to reduce systemic inflammation before stimulation begins, which may improve egg quality and endometrial conditions ahead of transfer.
The IVF process step by step for endometriosis
The endometriosis IVF process follows the same general phases as standard IVF, but with specific adaptations at each stage.
-
Baseline assessment and suppression. Your cycle begins with blood work and ultrasound to confirm your ovaries are quiet and free of large cysts. If a new endometrioma has appeared, your team will discuss whether to proceed or intervene.
-
Ovarian stimulation. You will self-inject gonadotropin medications for 8 to 12 days to stimulate multiple follicles. Monitoring appointments every 2 to 3 days track follicle size and estrogen levels. Women with endometriosis sometimes respond differently than expected, producing fewer eggs than their antral follicle count suggested, or responding unevenly across ovaries.
-
Trigger shot and egg retrieval. Once follicles reach the right size, a trigger injection finalizes maturation. Retrieval happens 36 hours later under light sedation. For women with endometriomas, the retrieval team will take extra precautions to avoid puncturing cyst walls, which can introduce fluid into the follicular environment and affect egg quality.
-
Fertilization and embryo culture. Retrieved eggs are fertilized in the laboratory, typically using ICSI (intracytoplasmic sperm injection) for more precise fertilization control. Embryos are cultured for 5 to 6 days to the blastocyst stage, where they can be assessed for quality and, if desired, tested genetically.
-
Embryo freezing (the freeze-all strategy). Here is where the endometriosis IVF process diverges most clearly from standard care. Rather than transferring an embryo in the same cycle as retrieval, most endometriosis specialists recommend freezing all viable embryos. This freeze-all approach allows the hormonal surge from stimulation to subside before transfer, creating a calmer uterine environment.
The benefits of the freeze-all strategy are well established:
- Reduced inflammatory response in the endometrium at the time of transfer
- Ability to time transfer during a more naturally stable hormonal window
- Lower risk of symptom flares triggered by high estrogen levels post-retrieval
- More time to assess embryo quality before committing to a transfer
- Frozen embryo transfer (FET). In a separate cycle weeks or months later, your endometrium is prepared with estrogen and progesterone. Once the lining reaches the target thickness, a single embryo is transferred. FET consistently produces higher clinical pregnancy and live birth rates than fresh transfer in endometriosis patients, which is a well-supported finding in current research.
Learn more about how this phase works at Lifeivfcenter’s detailed resource on frozen embryo transfer.
Success rates and outcomes based on endometriosis stage
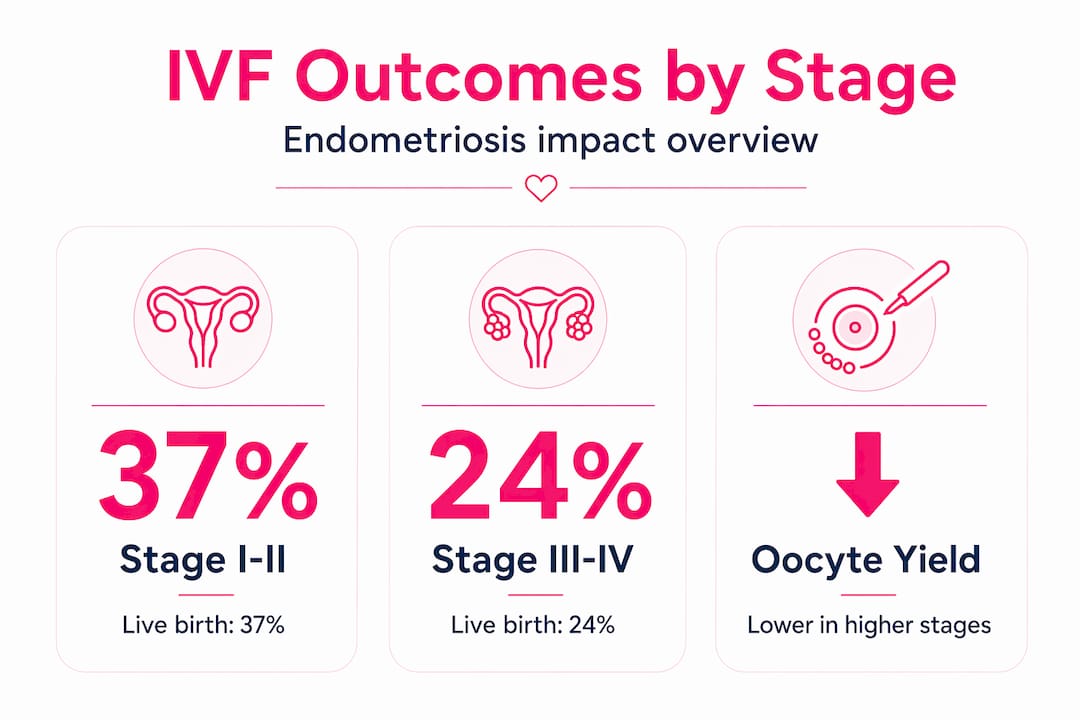
Understanding endometriosis and IVF success rates means accepting that the numbers vary considerably depending on disease severity, age, and ovarian reserve. Here is a realistic overview of what current data shows.
| Endometriosis stage | Oocyte yield | Clinical pregnancy rate | Live birth rate |
|---|---|---|---|
| Stage I to II (minimal to mild) | Comparable to controls | Similar to non-endometriosis patients | Generally favorable |
| Stage III to IV (moderate to severe) | Reduced, especially with endometriomas | Lower than stages I to II | Reduced vs. earlier stages |
The multifactorial nature of endometriosis means that stage alone does not determine your outcome. Your age at treatment, your AMH level, the number of prior surgeries on your ovaries, and the presence of additional infertility factors all contribute to your personal prognosis.
Several factors consistently influence outcomes beyond disease stage:
- Prior ovarian surgeries: Each procedure on an endometrioma reduces the functional ovarian tissue remaining. More surgeries correlate with lower egg yields.
- AMH and antral follicle count: These markers give the most direct read on how many eggs IVF is likely to retrieve.
- Endometrial receptivity: Even with good embryos, implantation can be affected by the same inflammation that defines endometriosis. FET timing strategies directly address this.
- Multidisciplinary care: Women who receive coordinated care from both a reproductive endocrinologist and a specialist in endometriosis pain management tend to have better overall outcomes.
Individualized IVF protocols consistently outperform standardized approaches in complex cases like endometriosis. The evidence supports tailoring stimulation and transfer strategies rather than applying a uniform protocol. Lifeivfcenter’s overview of endometriosis fertility strategies covers several evidence-based steps you can take to support your treatment outcomes.
My perspective on IVF with endometriosis
I have observed one consistent pattern across patients with endometriosis who go through IVF: the ones who do best are the ones who insist on a protocol built specifically for them. Not a standard protocol applied to their case. Their case, shaped into a protocol.
What I have learned is that timing is everything in this process. Rushing to transfer in the same cycle as retrieval, skipping the freeze-all strategy because it feels faster, or agreeing to surgery on an endometrioma just before IVF starts are the decisions I most often see patients regret. The data on frozen transfers for endometriosis is not ambiguous. A calmer endometrium responds better.
The emotional weight of managing a painful chronic condition while pursuing fertility is real and rarely gets enough clinical attention. Patients often come in already exhausted. Advocating for a protocol that accounts for your symptoms, your reserve, and your personal timeline is not difficult or demanding. It is medically reasonable. Do not accept a plan that treats your endometriosis as a footnote.
— Ben
How Lifeivfcenter supports endometriosis patients
At Lifeivfcenter, the approach to IVF for endometriosis starts with a thorough fertility evaluation and a protocol built around your biology, not a default treatment model. The clinic’s Precision IVF approach customizes stimulation, monitoring, and transfer timing based on your disease stage, ovarian reserve, and treatment history, which is exactly what current evidence recommends for complex cases.
For women exploring endometriosis fertility options, Lifeivfcenter offers embryo freezing, personalized FET planning, and access to fertility treatment packages designed to make advanced care accessible. If you are ready to understand what a tailored IVF plan could look like for your specific situation, Lifeivfcenter’s team is available to guide you through your options with the detail and compassion this process deserves.
FAQ
Does endometriosis lower IVF success rates?
Endometriosis affects IVF success rates depending on disease stage. Stages I and II show outcomes comparable to patients without endometriosis, while stages III and IV are associated with lower oocyte retrieval, clinical pregnancy, and live birth rates.
Is frozen embryo transfer better than fresh for endometriosis?
Yes. Meta-analyses consistently show that frozen embryo transfer produces higher clinical pregnancy and live birth rates in endometriosis patients, because the transfer occurs in a less inflamed, hormonally stabilized uterine environment.
Should I have surgery to remove an endometrioma before starting IVF?
Not necessarily. Current recommendations advise against operating on endometriomas before IVF unless the cyst is large enough to block egg retrieval, because surgery can reduce ovarian reserve. Your specialist should discuss fertility preservation options if surgery becomes necessary.
Which IVF protocol is best for endometriosis?
GnRH antagonist protocols are currently preferred for most endometriosis patients due to comparable success rates and a better safety profile compared to long agonist protocols. Gentler options like mini-IVF or PPOS may be appropriate depending on your ovarian reserve and symptom profile.
When should a woman with endometriosis consider IVF?
NICE guidelines suggest advancing to IVF after two years of failed expectant management or surgical treatment, though earlier consideration is appropriate when age, low ovarian reserve, or severe symptoms are present.
Recommended
- Evidence-Based Endometriosis Fertility Tips for Better Conception
- IVF Process Explained: Personalize Your Path to Success
- Understanding embryo transfer: The key step in IVF
- Egg retrieval tips: Expert guidance for IVF success
Ready to take the next step?
Life IVF Center specializes in individualized Precision IVF® care for complex cases—including diminished ovarian reserve, prior failed cycles, and advanced maternal age. Our in-house labs and dedicated physicians are ready to help.
Book a Free Consultation →