Mini IVF, clinically known as minimal stimulation IVF, is defined as a fertility treatment that uses low-dose oral medications and minimal injectable hormones to stimulate the ovaries to produce a small number of eggs. Knowing how to navigate the mini IVF protocol gives patients a real advantage: fewer surprises, better preparation, and clearer expectations at every stage. This guide walks through patient selection, preparation, the full cycle process, and how to handle common setbacks. Lifeivfcenter applies its Precision IVF® approach to tailor each mini IVF plan to the patient’s unique biology, history, and goals.
How to navigate the mini IVF protocol: who it is designed for
Mini IVF is most commonly indicated for patients with diminished ovarian reserve, those at high risk of ovarian hyperstimulation syndrome (OHSS), or patients who want to minimize their medication burden. This matters because the right protocol depends entirely on your biology, not on a one-size-fits-all standard.

Patient selection relies on two key ovarian reserve markers: anti-Müllerian hormone (AMH) and antral follicle count (AFC). A comprehensive evaluation that includes AMH, AFC, and full treatment history is the foundation for deciding between mini IVF and conventional IVF. Patients with low AMH or a low AFC often respond poorly to high-dose stimulation, making the gentler mini IVF approach a more practical fit.
Other factors that point toward mini IVF include:
- Prior poor response to conventional IVF stimulation protocols
- Elevated OHSS risk due to polycystic ovary syndrome (PCOS) or previous hyperstimulation
- Medication intolerance or sensitivity to high-dose injectable hormones
- Ethical preferences around limiting the number of embryos created
- Cost considerations, since lower medication volumes reduce overall cycle expense
One persistent misconception is that mini IVF produces higher-quality eggs than conventional IVF. Mini IVF does not inherently produce higher-quality eggs. The main trade-off is fewer embryos available per cycle, not better ones. Understanding this distinction helps patients set realistic expectations from the start.
Pro Tip: Before your first consultation, ask your doctor for your AMH level and AFC count. These two numbers will shape every protocol decision your care team makes. You can review how clinicians use these markers to select the right approach by reading about diminished ovarian reserve at Lifeivfcenter.
What does preparing for mini IVF actually involve?
Preparation for a mini IVF cycle starts with a complete fertility evaluation checklist that includes bloodwork, pelvic ultrasound, and semen analysis. These baseline tests confirm your starting point and flag any issues that need addressing before stimulation begins. Skipping or rushing this phase is the most common reason cycles get delayed.
Standard pre-cycle workup components include:
- Bloodwork: FSH, LH, estradiol, AMH, thyroid panel, and infectious disease screening
- Pelvic ultrasound: To assess AFC and uterine anatomy
- Semen analysis: To determine fertilization method, including whether intracytoplasmic sperm injection (ICSI) will be needed
- Medication review: Checking for supplements or prescriptions that may interfere with stimulation
Lifestyle preparation also matters. Reaching a healthy body weight, reducing alcohol, stopping smoking, and managing chronic stress all improve ovarian response. Your care team may recommend specific supplements such as CoQ10 or DHEA based on your ovarian reserve results, though supplement guidance should always come from your physician.
Mini IVF cycles require fewer monitoring visits than conventional IVF due to milder stimulation. Fewer clinic visits ease the scheduling burden, but each visit carries more weight. Missing a monitoring appointment can mean missing the optimal retrieval window.
Pro Tip: Set calendar alerts for every scheduled ultrasound and blood draw. Communicate any schedule conflicts to your care team at least 48 hours in advance. Open communication at this stage directly protects your cycle outcome.
What are the step-by-step stages of the mini IVF cycle?
The mini IVF process follows a clear sequence. Each stage builds on the last, and understanding what happens at each point reduces anxiety and improves your ability to respond quickly when your care team needs action from you.
-
Cycle day 1 confirmation: Your clinic confirms the start of your menstrual cycle and schedules your baseline ultrasound and bloodwork, typically on cycle day 2 or 3.
-
Ovarian stimulation: Clomiphene Citrate (Clomid) is the cornerstone oral medication used in mini IVF. It acts as a selective estrogen receptor modulator, increasing the body’s own FSH and LH to promote controlled follicular growth. Low-dose injectable gonadotropins are often added to support follicle development without pushing the ovaries into overdrive.
-
Monitoring phase: Ultrasound and hormone blood tests track follicle size and estradiol levels every few days. Mini IVF typically targets 1–5 mature follicles. The care team adjusts medication doses based on how your ovaries respond in real time.
-
Trigger shot: Once follicles reach the target size, the trigger shot, typically human chorionic gonadotropin (hCG), is administered. This induces final egg maturation approximately 36 hours before retrieval. Timing is critical. Administering the trigger too early or too late compromises egg maturity.
-
Egg retrieval: Mini IVF retrieval can be performed with lighter sedation than conventional IVF, often under local anesthesia or light sedation, due to the lower follicle count. Recovery is typically faster. The procedure uses a thin needle guided by ultrasound to aspirate eggs from the follicles.
-
Fertilization: Retrieved eggs are fertilized in the lab. ICSI, where a single sperm is injected directly into each egg, is frequently used when sperm quality is a concern or when egg numbers are limited. Your embryologist will confirm which method applies to your case.
-
Embryo culture and assessment: Fertilized eggs develop in the lab for 3–5 days. The embryology team monitors development and grades embryos based on quality. You can learn more about what to look for in signs of a healthy embryo at Lifeivfcenter.
-
Embryo transfer or freezing: One or two embryos are transferred to the uterus, typically on day 3 or day 5. Any remaining viable embryos are frozen for future use. Frozen embryo transfer cycles often follow in subsequent months if the fresh transfer does not result in pregnancy.
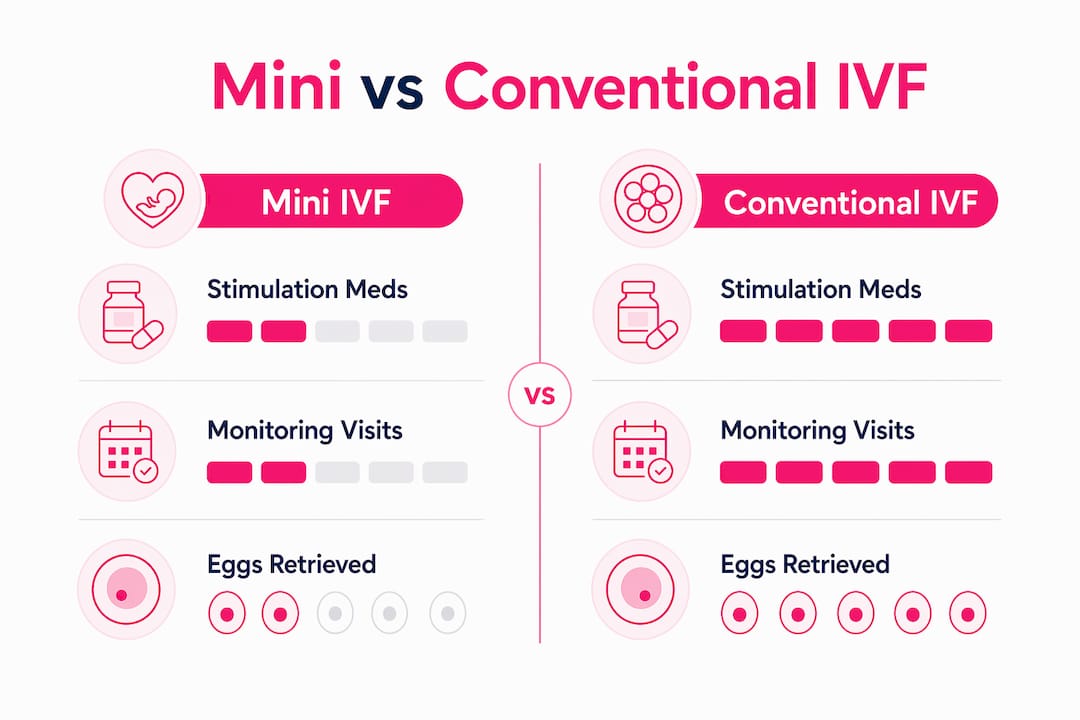
The table below compares mini IVF and conventional IVF across the key protocol stages.
| Protocol stage | Mini IVF | Conventional IVF |
|---|---|---|
| Stimulation medication | Clomid plus low-dose gonadotropins | High-dose injectable gonadotropins |
| Target follicle count | 1–5 follicles | 8–15+ follicles |
| Monitoring visits | Fewer visits required | Frequent visits required |
| Retrieval sedation | Local or light sedation | General anesthesia typical |
| Eggs retrieved per cycle | 1–5 eggs | 8–15+ eggs |
| OHSS risk | Significantly reduced | Higher risk |
Pro Tip: The trigger shot window is the most time-sensitive step in the entire cycle. Keep your phone accessible and confirm the exact injection time with your nurse the day before. A one-hour error can affect egg maturity.
What success rates and risks should you expect from mini IVF?
Success rates per cycle are lower with mini IVF than with conventional IVF because fewer eggs are retrieved. Patients may need several cycles of mini IVF to match the cumulative success rates of one conventional IVF cycle. This is the central trade-off patients must weigh before committing to the protocol.
Key risks and considerations include:
- Cycle cancellation: If no follicles develop adequately, the cycle may be canceled before retrieval
- Premature ovulation: Without suppression medications, eggs can release before retrieval, losing the cycle
- Lower embryo yield: Fewer eggs mean fewer embryos, which reduces the number of transfer attempts available
- OHSS risk is significantly lowered but not completely eliminated with mini IVF protocols
“The psychological impact of mini IVF can be significant. Emotional challenges arise due to lower egg yields and the possible need for multiple cycles. Adequate counseling and support improve outcomes and help patients stay the course when results take time.”
Patients who choose mini IVF because of ethical concerns about embryo numbers or cost factors often find the lower-yield approach more aligned with their values. That alignment supports emotional resilience through multiple cycles. Planning for the possibility of two or three cycles from the outset, rather than expecting one cycle to succeed, leads to better psychological preparation and more consistent follow-through.
How do you troubleshoot common challenges in the mini IVF process?
Poor ovarian response is the most frequent obstacle in mini IVF. Monitoring helps detect poor response early so clinics can avoid unnecessary procedures and modify future stimulation plans. If your follicles are not growing as expected, your care team will adjust medication doses or timing before canceling the cycle outright.
Common challenges and practical responses:
- Slow follicle growth: Your physician may add low-dose gonadotropin injections mid-cycle to support development
- Medication side effects: Clomid can cause hot flashes, mood changes, and visual disturbances. Report any visual symptoms immediately. Most other side effects are mild and resolve after the stimulation phase ends
- Cycle cancellation: If a cycle is canceled, use the recovery period to review what the monitoring data showed. That information directly shapes the next protocol adjustment
- Scheduling conflicts with monitoring: Missing an ultrasound during the monitoring window can mean missing the retrieval window entirely. Prioritize these appointments above all others
- Emotional fatigue: Multiple cycles are common. Connecting with a counselor or a peer support group between cycles maintains psychological resilience
Flexible planning is not a sign of failure. It is the standard operating mode for mini IVF. Clinics that specialize in this protocol expect to refine the approach across cycles, and patients who understand this from the start adapt more effectively when adjustments are needed.
Key Takeaways
Mini IVF is the right protocol for specific patient profiles, and success depends on preparation, precise timing, and realistic expectations across multiple cycles.
| Point | Details |
|---|---|
| Patient selection is critical | AMH and AFC results, not personal preference alone, determine whether mini IVF is the right protocol. |
| Preparation protects the cycle | Complete bloodwork, ultrasound, and semen analysis before stimulation begins to avoid mid-cycle surprises. |
| Trigger shot timing is decisive | Administer hCG within the exact window your care team specifies; a timing error directly affects egg maturity. |
| Plan for multiple cycles | Per-cycle success rates are lower than conventional IVF; cumulative rates improve with each additional attempt. |
| Emotional support is part of the protocol | Counseling and peer support between cycles improve adherence and psychological resilience. |
What I have learned from guiding patients through mini IVF
The patients who do best with mini IVF are not the ones who chose it because it sounded easier. They are the ones who understood the trade-offs clearly before they started. Lower medication burden is real. Lower per-cycle success rates are equally real. Patients who hold both truths at once tend to stay committed through the process.
The detail that surprises most patients is how much the trigger shot timing matters relative to everything else in the cycle. I have seen well-prepared patients lose a cycle to a timing error that could have been avoided with a single phone confirmation. That one step deserves more attention than it typically gets in general guides.
The other pattern worth naming is that mini IVF works best as a planned multi-cycle strategy, not a single attempt. Clinics that communicate this clearly from the first consultation see better patient outcomes, not because the biology changes, but because patients who expect multiple cycles do not abandon the protocol after one difficult result. Effective communication and managing patient expectations throughout mini IVF cycles improves adherence and psychological resilience when multiple cycles are needed. That finding reflects what I observe in practice every time.
— Ben
How Lifeivfcenter supports patients through every mini IVF stage
Lifeivfcenter applies its Precision IVF® approach to every mini IVF cycle, customizing stimulation protocols based on each patient’s AMH, AFC, age, and treatment history. No two protocols are identical because no two patients are identical.
Patients at Lifeivfcenter’s Southern California locations receive individualized monitoring schedules, direct access to their care team, and clear guidance at every decision point in the cycle. The clinic’s fertility treatment packages are structured to make mini IVF financially accessible without compromising clinical quality. For patients who want to understand the full scope of what Lifeivfcenter offers before booking a consultation, the overview of care page covers the clinic’s full range of reproductive services. Scheduling a consultation is the first step toward a protocol built around your specific biology.
FAQ
What is mini IVF and how does it differ from conventional IVF?
Mini IVF uses low-dose oral medications, primarily Clomiphene Citrate, plus minimal injectable hormones to retrieve a small number of eggs. Conventional IVF uses high-dose injectables to produce 8–15 or more eggs per cycle, resulting in higher per-cycle success rates but greater OHSS risk.
Who is the best candidate for mini IVF?
Patients with diminished ovarian reserve, high OHSS risk, medication intolerance, or ethical concerns about creating large numbers of embryos are the strongest candidates. AMH and AFC results guide this decision more than any other single factor.
How many monitoring visits does mini IVF require?
Mini IVF requires fewer monitoring visits than conventional IVF because stimulation is milder. Patients typically attend two to four ultrasound and blood test appointments during the stimulation phase, though exact frequency depends on individual response.
Can mini IVF succeed on the first cycle?
Yes, but per-cycle success rates are lower than conventional IVF. Patients should plan for the possibility of multiple cycles. Cumulative pregnancy chances increase meaningfully with each additional attempt, particularly when the protocol is adjusted based on prior cycle data.
What happens if a mini IVF cycle is canceled?
If follicles do not respond adequately, the cycle is canceled before retrieval to avoid unnecessary procedures. The monitoring data from that cycle directly informs adjustments to the next stimulation plan, making each canceled cycle a source of useful clinical information. You can also review how to manage IVF side effects and what to expect during recovery at Lifeivfcenter.
Recommended
- IVF Process Explained: Personalize Your Path to Success
- The IVF Process – Life IVF Center
- Pre-IVF Requirements – Life IVF Center
- Frequently Asked Questions – Life IVF Center
Ready to take the next step?
Life IVF Center specializes in individualized Precision IVF® care for complex cases—including diminished ovarian reserve, prior failed cycles, and advanced maternal age. Our in-house labs and dedicated physicians are ready to help.
Book a Free Consultation →