
Most people assume fertility testing is something you pursue only after months or years of failed attempts to conceive. That assumption can cost you time, options, and emotional energy. Infertility affects 1 in 8 couples, and male factors contribute to 40 to 50% of those cases, meaning both partners carry real risk from the start. Understanding your reproductive health before problems arise is not an overreaction. It is a practical, evidence-based decision that gives you more control over your family planning timeline and treatment choices.
Table of Contents
- The realities of infertility: Prevalence and overlooked factors
- Why timing matters: Understanding age, ovarian reserve, and fertility decline
- What fertility testing involves: Key tests and what they reveal
- How early testing informs your next steps and options
- Why proactive fertility testing is the best investment in your family future
- Get expert support for your fertility journey
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Infertility is common | Both women and men can face fertility challenges, making testing relevant for most couples hoping to conceive. |
| Timing is critical | Fertility declines with age, so early testing means more options and higher success rates. |
| Testing covers both partners | A thorough evaluation looks at male and female factors to ensure no causes are missed. |
| Testing empowers choices | Knowing your results helps you plan, whether for natural conception, fertility treatment, or preservation. |
| Professional support matters | Guided testing and expert advice lead to better outcomes and less uncertainty in your fertility journey. |
The realities of infertility: Prevalence and overlooked factors
Many people still think of infertility as a rare condition that happens to someone else. The data tells a very different story. Infertility affects 1 in 8 couples, and the causes are split more evenly between men and women than most people expect. Male factors account for 40 to 50% of infertility cases, which means limiting testing to women alone leaves half the picture unexamined.
Female infertility has also been rising at a significant rate globally. Global female infertility prevalence rose 84% between 1990 and 2021, reaching 110 million cases worldwide. The age group carrying the highest burden is women ages 35 to 39. This trend reflects delayed family planning, lifestyle factors, and underlying conditions that often go undetected without proactive screening.
| Factor | Female contribution | Male contribution |
|---|---|---|
| Infertility cases | 50 to 60% | 40 to 50% |
| Age-related decline begins | Early 30s | Mid to late 30s |
| Highest burden age group | 35 to 39 | 40 and older |
| Most common conditions | PCOS, endometriosis, POI | Varicocele, low sperm count |
Several myths still circulate that discourage early testing:
- “We’re young, so we don’t need testing.” Age is one factor, but structural issues, hormonal imbalances, and genetic conditions affect people of all ages.
- “If something were wrong, we’d know it.” Most fertility-related conditions produce no obvious symptoms. PCOS, low sperm count, and diminished ovarian reserve are often silent.
- “Testing is only for women.” As the data shows, male factors are responsible for nearly half of all cases. Reviewing male fertility tips is a practical starting point for any couple.
- “We’ll try naturally first and test later.” Waiting without information can narrow your options, particularly if age-related decline is already underway.
“Early evaluation is not about assuming something is wrong. It is about knowing where you stand so you can make decisions that reflect your actual biology, not your assumptions about it.”
The takeaway is straightforward: fertility testing is not a last resort. It is a first step toward informed family planning, and it applies equally to both partners.
Why timing matters: Understanding age, ovarian reserve, and fertility decline
Age is the single most predictable factor affecting fertility outcomes. For women, ovarian reserve, meaning the quantity and quality of remaining eggs, begins declining in the early 30s and accelerates after 35. This decline is not reversible, and it happens regardless of general health or fitness level.
The most reliable single marker for ovarian reserve is Anti-Müllerian Hormone, or AMH. AMH assesses ovarian reserve, and low levels, typically below 1.2 ng/mL, often indicate diminished ovarian reserve (DOR). Low AMH also predicts a poor response to ovarian stimulation during IVF, particularly in women over 35. AMH levels decline steadily with age, making early measurement especially valuable for planning.
IVF success rates reflect this age-related decline clearly. IVF success drops sharply with age: women under 35 achieve approximately 50% success per cycle, dropping to around 38% at ages 35 to 37, roughly 24% at ages 38 to 40, and below 15% using their own eggs after age 40.
How to interpret key fertility markers by age:
- Under 30: AMH is typically robust; testing establishes a useful baseline and identifies hidden conditions early.
- 30 to 34: A good window for proactive testing; reserve is still adequate for most, but trends are informative.
- 35 to 37: Decline accelerates; testing at this stage is urgent if conception is planned within 1 to 2 years.
- 38 to 40: Options narrow quickly; results should directly inform whether to pursue treatment immediately.
- Over 40: Egg quality and quantity are significantly reduced; donor egg options may be discussed alongside own-egg protocols.
Male fertility also declines with age, though more gradually. Sperm DNA fragmentation increases after age 40, raising miscarriage risk and reducing fertilization rates. Both partners benefit from early evaluation, not just the female partner.
Pro Tip: AMH is just one piece of the picture. Ask your fertility specialist to combine it with antral follicle count (AFC) from an ultrasound and FSH (follicle-stimulating hormone) for a more complete view of your ovarian reserve. You can learn more about understanding low AMH and what it means for your treatment options, and review the diminished ovarian reserve guide if your results come back lower than expected.
The core message here is that time is a variable you cannot recover. Testing early gives you the information needed to act while your options are still broad.
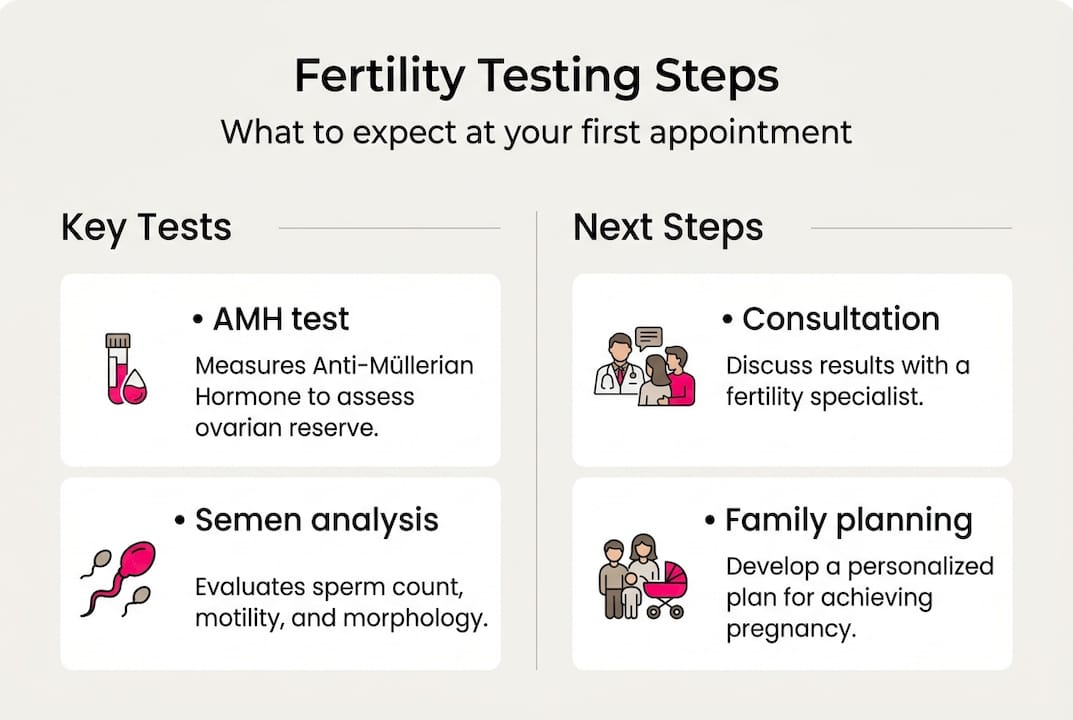
What fertility testing involves: Key tests and what they reveal
Fertility testing is far less intimidating than most people expect. For the majority of patients, the initial workup involves a blood draw and an ultrasound for women, and a semen analysis for men. These foundational tests reveal a significant amount of information and guide whether further investigation is needed.
For women, standard fertility testing typically includes:
- AMH blood test: Measures ovarian reserve; results guide stimulation protocols if IVF is considered.
- FSH and estradiol on cycle day 3: Elevated FSH can signal declining reserve or poor ovarian function.
- Antral follicle count (AFC): A transvaginal ultrasound counts visible follicles, offering a direct visual of reserve.
- Thyroid function and prolactin: Hormonal imbalances in these areas can disrupt ovulation and implantation.
- Hysterosalpingogram (HSG): An X-ray procedure that checks whether the fallopian tubes are open and the uterine cavity is normal.
For men, testing begins with semen analysis, which evaluates:
- Sperm count (concentration)
- Motility (percentage of moving sperm)
- Morphology (shape and structure)
- Volume and pH of the sample
If semen analysis results are abnormal, follow-up testing may include hormone panels (FSH, LH, testosterone), genetic screening, or advanced diagnostics like sperm DNA fragmentation analysis. Reviewing male testing FAQs can help men understand what to expect and how to prepare.
Edge cases require additional attention. Conditions like polycystic ovary syndrome (PCOS) often produce elevated AMH, while premature ovarian insufficiency (POI) may require AMH when FSH results are inconclusive. Men with varicocele, an enlargement of veins in the scrotum, may need imaging alongside semen analysis. Patients with a history of cancer treatment, including chemotherapy or radiation, require a modified testing approach that accounts for treatment-related effects on reproductive tissue.
“Approximately 30% of infertility cases are classified as unexplained after a standard workup. Even in these cases, empiric treatment, meaning treatment based on clinical judgment rather than a confirmed diagnosis, remains a viable and often successful path forward.” Guidelines from NHS, ASRM, and WHO support this approach consistently.
The fertility consultation guide at Life IVF Center outlines what your first appointment will cover, and the pre-IVF checklist helps you prepare if testing suggests moving toward assisted reproduction.
Pro Tip: Bring a list of any medications, supplements, or prior diagnoses to your first fertility appointment. Conditions like thyroid disorders, autoimmune diseases, or prior surgeries can all influence test interpretation and treatment planning.
How early testing informs your next steps and options
Fertility test results are not just numbers on a page. They are decision-making tools. Depending on what your results show, your next steps could range from simple lifestyle adjustments to structured fertility treatment, and knowing early gives you the widest range of choices.
Early testing is crucial because age-related fertility decline makes timing a central factor in both natural conception and assisted reproductive technology (ART). Acting on information sooner rather than later preserves your options in meaningful ways.
How results typically translate into action:
- Normal results: Reassurance that natural conception is a reasonable approach; lifestyle optimization and a defined timeline for follow-up if conception does not occur.
- Mild abnormalities: Targeted interventions such as ovulation induction with oral medications, intrauterine insemination (IUI), or dietary and lifestyle changes.
- Significant findings (low AMH, poor semen analysis, blocked tubes): Direct referral to IVF or other ART options, with a treatment protocol tailored to your specific profile.
- Fertility preservation indicated: If you are not ready to conceive now but results suggest declining reserve, egg or sperm freezing may be the most strategic choice. Reviewing fertility preservation options can help you understand costs and timing.
- Unexplained infertility: Empiric treatment protocols, including IUI or IVF, are recommended based on clinical experience and your age-related risk profile.
| Test result | Likely next step | Time sensitivity |
|---|---|---|
| Normal reserve, normal semen | Timed natural conception | Low to moderate |
| Low AMH, normal semen | IVF with own eggs, possible banking | High |
| Blocked tubes | IVF bypasses tubes entirely | High |
| Abnormal semen analysis | Repeat test, urologist referral | Moderate to high |
| Unexplained infertility | IUI or IVF based on age | Age-dependent |
Understanding the intro to IVF process early helps you make decisions without feeling rushed. When you have results in hand, conversations with your care team become specific and productive rather than general and speculative.
Pro Tip: If your results suggest fertility preservation is wise, do not wait for a “perfect time” to freeze eggs or sperm. Ovarian reserve does not pause while you decide. Acting within the next cycle or two can make a measurable difference in the quality and quantity of what is preserved.
Why proactive fertility testing is the best investment in your family future
There is a perspective that is rarely stated plainly in fertility medicine, but it is one that experience consistently supports: almost no one regrets testing early, and many people deeply regret waiting. This is not a fear-based argument. It is a practical one rooted in how biology and time interact.
Guidelines from NHS, ASRM, and WHO all converge on the same recommendation: evaluate both partners early, start with foundational tests, and move systematically. The consensus across major medical bodies is not ambiguous. There is no credible clinical argument for delaying evaluation when someone is actively considering parenthood.
What the guidelines do not fully capture is the emotional dimension. Patients who test early and find normal results gain something valuable: peace of mind and a clear timeline. Patients who test early and find issues gain something equally valuable: time to act. The patients who struggle most are often those who waited, assuming everything was fine, only to discover a significant issue when their options had already narrowed.
Consider two scenarios. A 33-year-old woman tests proactively and discovers low AMH. She has time to pursue IVF with her own eggs, freeze embryos, and complete her family on a planned timeline. A 38-year-old woman in the same situation, who delayed testing, may face a compressed window, reduced egg quality, and a harder emotional journey. The biology is identical. The outcomes differ because of timing.
This is why proactive testing is not just a medical recommendation. It is an act of self-advocacy. Reading real fertility success stories from patients who navigated similar decisions can reinforce that early action leads to better outcomes, both medically and emotionally.
The field has moved well beyond the idea that fertility care is only for people in crisis. It is for anyone who wants to make informed, empowered decisions about when and how they build their family.
Get expert support for your fertility journey
Taking the step from reading about fertility testing to actually scheduling an evaluation is where clarity begins. Life IVF Center provides personalized fertility evaluations that go beyond standard testing, incorporating each patient’s full medical history, hormonal profile, and family goals into a tailored plan.
If you are unsure whether your insurance covers fertility testing, the insurance for fertility testing page outlines what many plans include and how to navigate coverage questions before your first appointment. For those ready to explore treatment, Precision IVF options at Life IVF Center are designed to maximize success rates by customizing every protocol to your unique biology. You can also attend a fertility webinar to get answers to your questions in a low-pressure, educational setting before committing to an in-person visit. Your next step does not have to be complicated. It just has to be a step.
Frequently asked questions
When should you consider fertility testing?
You should consider fertility testing if you have been trying to conceive for 12 months without success, or 6 months if you are over 35. Known risk factors like PCOS, endometriosis, irregular cycles, or prior cancer treatment also warrant earlier evaluation, per guidelines from NHS, ASRM, and WHO.
Does fertility testing hurt?
Most fertility tests involve a blood draw or semen analysis and are not painful. A transvaginal ultrasound or HSG procedure may cause mild discomfort, but both are brief and routinely performed in outpatient settings.
What is AMH and why does it matter?
AMH (Anti-Müllerian Hormone) reflects how many eggs remain in your ovaries and predicts how your body will respond to IVF stimulation. Low AMH levels below 1.2 ng/mL often indicate diminished ovarian reserve and signal the need for timely treatment decisions.
Can men benefit from fertility testing too?
Absolutely. Male factors contribute to 40 to 50% of infertility cases, making semen analysis an essential part of any couple’s evaluation. Testing both partners from the start prevents delays caused by incomplete information.
Recommended
- A. Intro to IVF Archives – Life IVF Center
- Fertilization & Culturing – Life IVF Center
- Male Fertility: Tips and Key Factors for IVF Success – Life IVF Center
- Egg and Embryo Freezing – Fertility Preservation Packages
Ready to take the next step?
Life IVF Center specializes in individualized Precision IVF® care for complex cases—including diminished ovarian reserve, prior failed cycles, and advanced maternal age. Our in-house labs and dedicated physicians are ready to help.
Book a Free Consultation →