Female infertility is defined as the inability to conceive after 12 months of regular, unprotected sex for women under 35, or after 6 months for women 35 and older. This clinical distinction matters because age changes the urgency of evaluation. Approximately 15% of couples worldwide experience infertility, making it one of the most common reproductive health concerns. Female infertility explained clearly and early gives women the best chance to act before time becomes a limiting factor. The World Health Organization and the National Institutes of Health both recognize infertility as a medical condition requiring structured diagnosis and care.
What are the primary causes of female infertility?
Ovulatory dysfunction accounts for 25% to 40% of female infertility cases. That makes it the single most common category. Polycystic ovary syndrome, or PCOS, is responsible for about 70% of anovulatory infertility. PCOS disrupts the hormonal signals that trigger ovulation, which means eggs are not released consistently or at all.
Tubal factor infertility contributes to 20% to 35% of cases. Blocked or damaged fallopian tubes prevent sperm from reaching the egg. The most common causes include pelvic inflammatory disease, prior pelvic surgeries, and endometriosis. Endometriosis alone can cause scarring that distorts the tubes and ovaries, reducing the chance of natural conception. Women dealing with this condition can find detailed guidance on managing endometriosis and fertility.

Uterine causes, including fibroids, polyps, and congenital anomalies, account for roughly 10% to 15% of cases. These structural issues can interfere with implantation even when ovulation and fertilization occur normally. Congenital anomalies like a septate uterus are often discovered only during a fertility workup.
Lifestyle factors also play a measurable role in reproductive health:
- Weight: Both obesity and being underweight disrupt hormonal balance and ovulation. Excess body fat raises estrogen levels, while very low body fat suppresses the hormones needed to trigger ovulation.
- Smoking: Tobacco use accelerates egg loss and damages the genetic material inside eggs. The effect is dose-dependent and not fully reversible.
- Alcohol: Excessive alcohol consumption reduces ovarian reserve and disrupts the menstrual cycle.
- Environmental toxins: Exposure to pesticides, plastics, and industrial chemicals can interfere with hormone signaling. This is an area of growing clinical concern.
Pro Tip: If you have irregular periods, significant pelvic pain, or a history of pelvic infections, bring those details to your first fertility appointment. These signs of female infertility often point directly to a diagnosable cause.
How is female infertility diagnosed?
A structured diagnostic process is the foundation of effective treatment. Clinicians follow a defined sequence to identify the cause before recommending any intervention.
- Medical history and physical exam. The physician reviews menstrual cycle patterns, prior pregnancies, surgeries, infections, and medications. A pelvic exam checks for structural abnormalities.
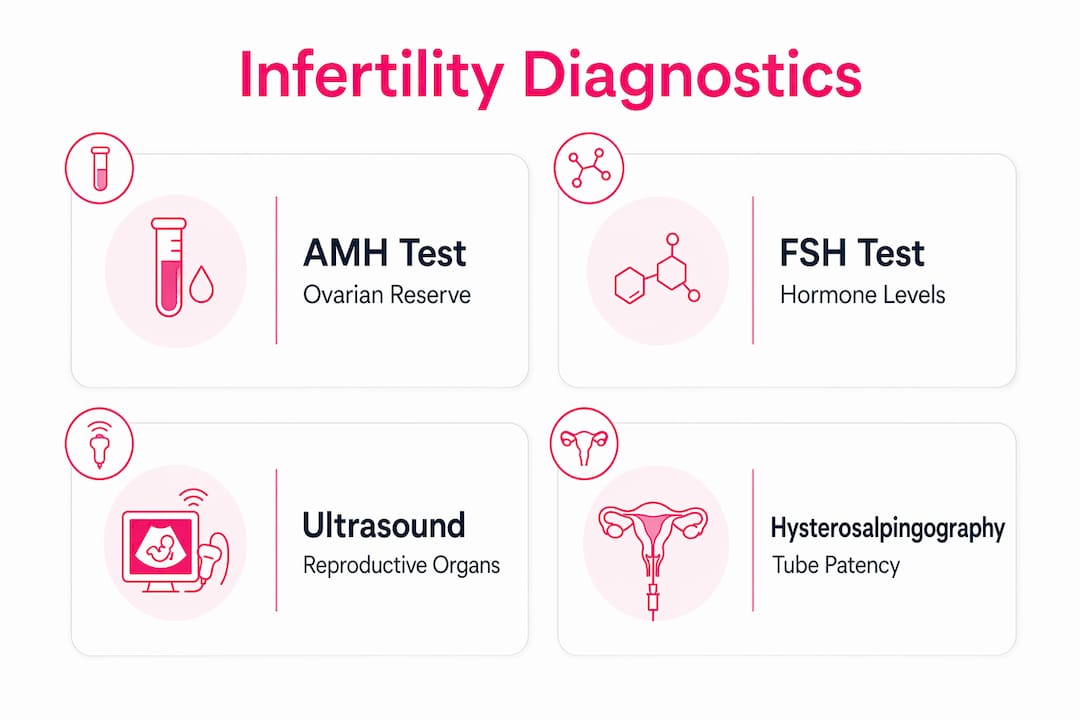
- Hormonal blood tests. Key markers include anti-Müllerian hormone (AMH) to assess ovarian reserve, follicle-stimulating hormone (FSH) to evaluate pituitary signaling, thyroid-stimulating hormone (TSH) to rule out thyroid disorders, and prolactin to detect hormonal imbalances that suppress ovulation.
- Imaging studies. A hysterosalpingogram (HSG) uses contrast dye and X-ray to check whether the fallopian tubes are open and the uterine cavity is normal. Transvaginal ultrasound assesses ovarian follicle count and uterine structure. Hysterosonography uses saline infusion to detect polyps or fibroids inside the uterus.
- Laparoscopy. When imaging is inconclusive, a minimally invasive surgical procedure allows direct visualization of the pelvis to identify endometriosis or adhesions.
Understanding why fertility testing matters helps patients approach this process with clarity rather than anxiety.
Unexplained infertility is a diagnosis of exclusion. It applies when all standard tests return normal results. Unexplained infertility affects 15% to 30% of patients who complete a full workup. This does not mean nothing is wrong. It means current diagnostics have not yet identified the cause. Research is actively working to close that gap.
| Diagnostic test | What it measures |
|---|---|
| AMH blood test | Ovarian reserve and egg supply |
| FSH blood test | Pituitary hormone signaling to ovaries |
| HSG imaging | Fallopian tube patency and uterine shape |
| Transvaginal ultrasound | Follicle count, ovarian cysts, uterine structure |
| Laparoscopy | Direct visualization of endometriosis or adhesions |
Pro Tip: Before your first fertility appointment, log at least three months of menstrual cycle data, including cycle length, flow, and any pain. Documenting cycle regularity and past medical events helps clinicians reach a diagnosis faster.
What treatment options are available for female infertility?
Treatment for female infertility is matched to the identified cause. There is no single protocol that works for every patient. The most effective approach depends on age, diagnosis, ovarian reserve, and personal goals.
Ovulation induction is the first-line treatment for women with ovulatory dysfunction. Letrozole is preferred over clomiphene citrate for PCOS-related anovulation, based on WHO 2026 guidelines. Letrozole produces higher ovulation and live birth rates with fewer multiple pregnancy risks. Metformin may be added when insulin resistance is present. When oral medications fail, injectable gonadotropins are the next step.
Surgical interventions address structural causes directly:
- Hysteroscopic surgery removes fibroids or polyps inside the uterine cavity.
- Laparoscopic surgery treats endometriosis, removes adhesions, and can repair damaged tubes in selected cases.
- Uterine septum resection corrects congenital anomalies that interfere with implantation.
Assisted reproductive technologies (ART) include intrauterine insemination (IUI) and in vitro fertilization (IVF). IUI places prepared sperm directly into the uterus around ovulation. IVF retrieves eggs, fertilizes them in a laboratory, and transfers embryos into the uterus. IVF is recommended when tubes are blocked, when ovulation induction fails, or when age-related decline makes time a critical factor. Lifeivfcenter’s Precision IVF approach customizes each protocol based on a patient’s biological profile, aiming to reduce unnecessary cycles.
Lifestyle modifications support treatment outcomes across all categories:
- Reaching a healthy body weight before treatment improves ovulation rates and embryo implantation.
- Stopping smoking before any ART cycle protects egg quality.
- Reducing alcohol consumption supports hormonal balance throughout treatment.
- Addressing environmental toxin exposure, where possible, reduces background hormonal disruption.
A full overview of fertility treatment options and their appropriate uses is available for patients who want to compare approaches before their consultation.
How do age and lifestyle factors affect fertility outcomes?
Age is the most powerful biological variable in female fertility. Fertility decline begins around age 30 and accelerates significantly by 35. Egg quantity and quality both decrease, and the rate of chromosomal abnormalities in eggs rises. This is why the clinical threshold for evaluation drops from 12 months to 6 months for women 35 and older.
Women 35 and older should not wait a full year before seeking evaluation. Six months of trying without success is the clinical trigger for a workup. Earlier assessment preserves more treatment options and improves outcomes.
Lifestyle factors compound the effects of age. Weight management, smoking cessation, and reduced alcohol each independently improve fertility and treatment success rates. Environmental toxins add a layer of risk that is harder to control but worth addressing. Reducing exposure to endocrine-disrupting chemicals in food packaging, personal care products, and workplace environments supports hormonal health.
Age-related fertility factors are well documented, and understanding them helps patients seek timely intervention without unnecessary fear. Knowledge converts into better timing, and better timing converts into better outcomes.
Key Takeaways
Female infertility has identifiable causes in the majority of cases, and early, structured evaluation leads to faster, more effective treatment.
| Point | Details |
|---|---|
| Clinical definition matters | Seek evaluation after 12 months under 35, or 6 months at 35 and older. |
| Ovulatory dysfunction is the leading cause | PCOS drives 70% of anovulatory infertility and responds well to letrozole. |
| Diagnosis follows a defined sequence | AMH, FSH, HSG, and ultrasound together identify most structural and hormonal causes. |
| Unexplained infertility is not a dead end | 15%–30% of cases remain unexplained after testing; treatment can still succeed. |
| Lifestyle changes improve outcomes | Weight, smoking, and alcohol all affect both natural fertility and ART success rates. |
What I’ve learned from watching patients navigate this process
The women who do best in fertility treatment are not always the ones with the simplest diagnoses. They are the ones who came in informed, asked direct questions, and did not wait until they were exhausted by uncertainty to seek help.
One pattern I have seen repeatedly: patients who delayed evaluation because they assumed irregular cycles were normal. Irregular cycles are often the clearest early signal of ovulatory dysfunction. PCOS, thyroid disorders, and elevated prolactin all show up in cycle irregularity before they show up anywhere else. Treating that signal as background noise costs time that cannot be recovered.
The emotional weight of unexplained infertility is real and often underestimated. When every test comes back normal, patients frequently internalize the result as a personal failure. It is not. Unexplained infertility reflects the limits of current diagnostics, not the limits of the patient. Framing it that way changes how people engage with treatment, and engagement matters.
The advances in personalized IVF protocols over the past decade are genuinely significant. Matching stimulation protocols to individual ovarian reserve, genetic testing of embryos before transfer, and adjusting timing based on endometrial receptivity have all improved outcomes in ways that were not possible 15 years ago. Optimism in this field is grounded in real data, not reassurance.
— Ben
Personalized fertility care at Lifeivfcenter
Understanding the causes and options is the first step. Taking action with the right clinical team is what moves the process forward.
Lifeivfcenter offers affordable fertility treatment packages designed to match each patient’s diagnosis, age, and financial situation. The clinic’s Precision IVF® approach builds a customized protocol around your specific hormonal profile and medical history, reducing unnecessary cycles and improving the path to conception. Patients navigating insurance coverage can find dedicated support through the prospective insurance patients page. Consultations are available across multiple Southern California locations. If you are ready to move from information to action, Lifeivfcenter’s team is prepared to guide you through every step of the evaluation and treatment process.
FAQ
What is the medical definition of female infertility?
Female infertility is the inability to conceive after 12 months of regular, unprotected sex for women under 35, or after 6 months for women 35 and older. This time-based definition guides when clinical evaluation should begin.
What is the most common cause of female infertility?
Ovulatory dysfunction is the most common cause, accounting for 25% to 40% of cases. PCOS drives approximately 70% of ovulatory infertility and is typically treatable with medications like letrozole.
What does unexplained infertility mean?
Unexplained infertility means all standard diagnostic tests returned normal results. It affects 15% to 30% of patients and reflects the current limits of diagnostic tools, not the absence of a treatable condition.
How do doctors diagnose infertility in women?
Diagnosis includes a medical history review, hormonal blood tests (AMH, FSH, TSH, prolactin), and imaging studies such as HSG and transvaginal ultrasound. A GP referral can initiate the process, and fertility testing referrals follow a structured pathway.
At what age does female fertility start to decline?
Fertility decline begins around age 30 and accelerates significantly by 35. Women 35 and older are advised to seek evaluation after just 6 months of trying, rather than waiting the standard 12 months.
Recommended
- Real Examples of Fertility Challenges Explained
- Evidence-Based Endometriosis Fertility Tips for Better Conception
- Immunological Factors in Fertility: What You Need to Know
- Immune Disorder Fertility Solutions: Your Treatment Guide
Ready to take the next step?
Life IVF Center specializes in individualized Precision IVF® care for complex cases—including diminished ovarian reserve, prior failed cycles, and advanced maternal age. Our in-house labs and dedicated physicians are ready to help.
Book a Free Consultation →